
Intraocular Helminth
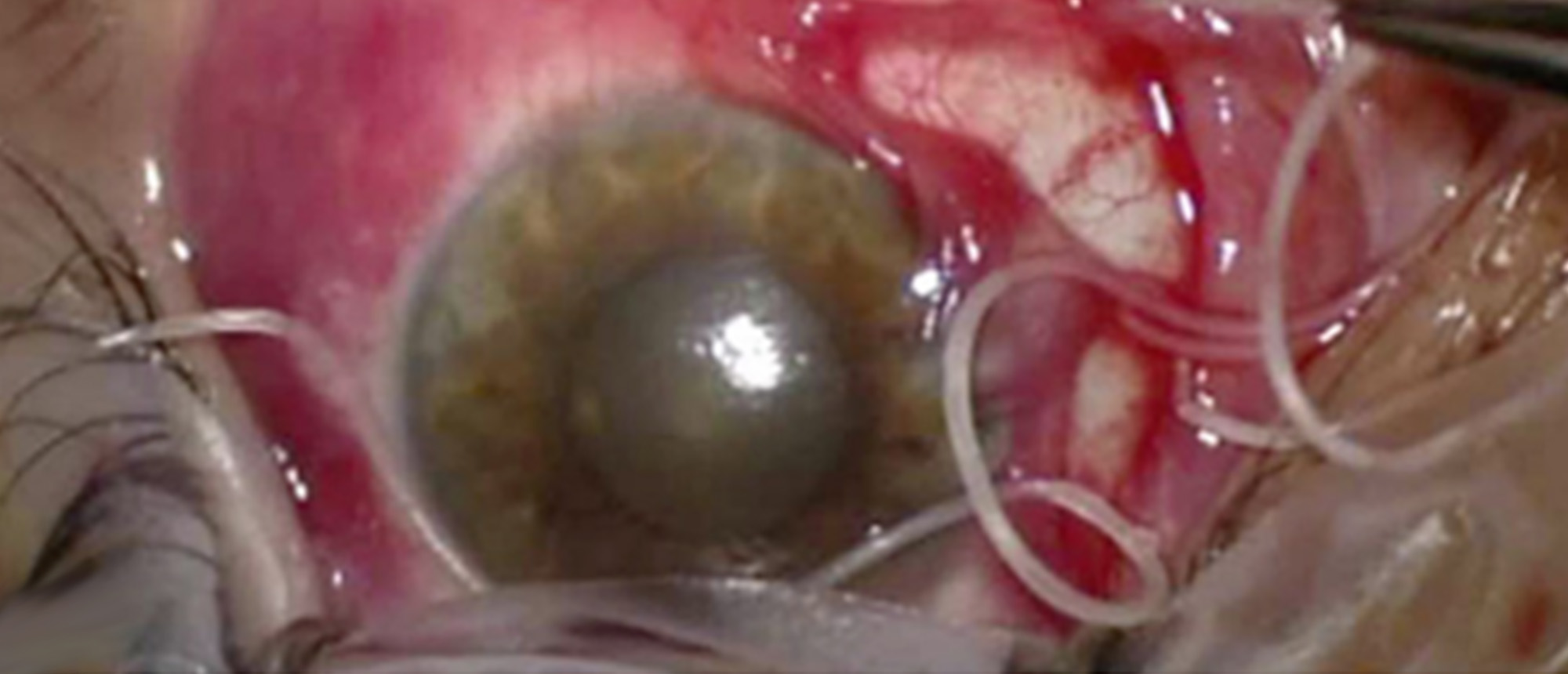
A middle-aged patient with past medical history significant for HIV (well-controlled on bictegravir, emtricitabine, and tenofovir) and history of Monkeypox infection presents to the emergency room complaining of foreign body sensation, redness, and itchiness in his right eye for two days. Visual acuity is 20/30 OD with pinhole measurement 20/25, and 20/40 with pinhole measurement to 20/20 OS. Intraocular pressures are normal, pupils are equal and reactive without an afferent pupillary defect. Slit lamp examination of the right eye is significant for temporal injection and elevation of the conjunctiva. When the light beam is shown on the affected area, an intraocular parasite is seen moving in the subconjunctival space. Posterior examination and left eye examination are otherwise unremarkable. The patient is diagnosed with a subconjunctival helminth. Subconjunctival 1% lidocaine with epinephrine is injected to paralyze the worm and block point of exit deeper into the orbit. A peritomy is performed with extraction of the subconjunctival parasite, with care taken to keep the parasite in one large piece. The patient was started on Albendazole therapy and given outpatient infectious disease follow up. At ophthalmology follow up five days later, and again 3 weeks later, the patient’s visual acuity remained unchanged, he denied further foreign body sensation or new acute symptoms.
Presentation Date: 12/12/2024
Issue Date: 02/14/2025
Please log in or click on ENROLL ME to access this course.
