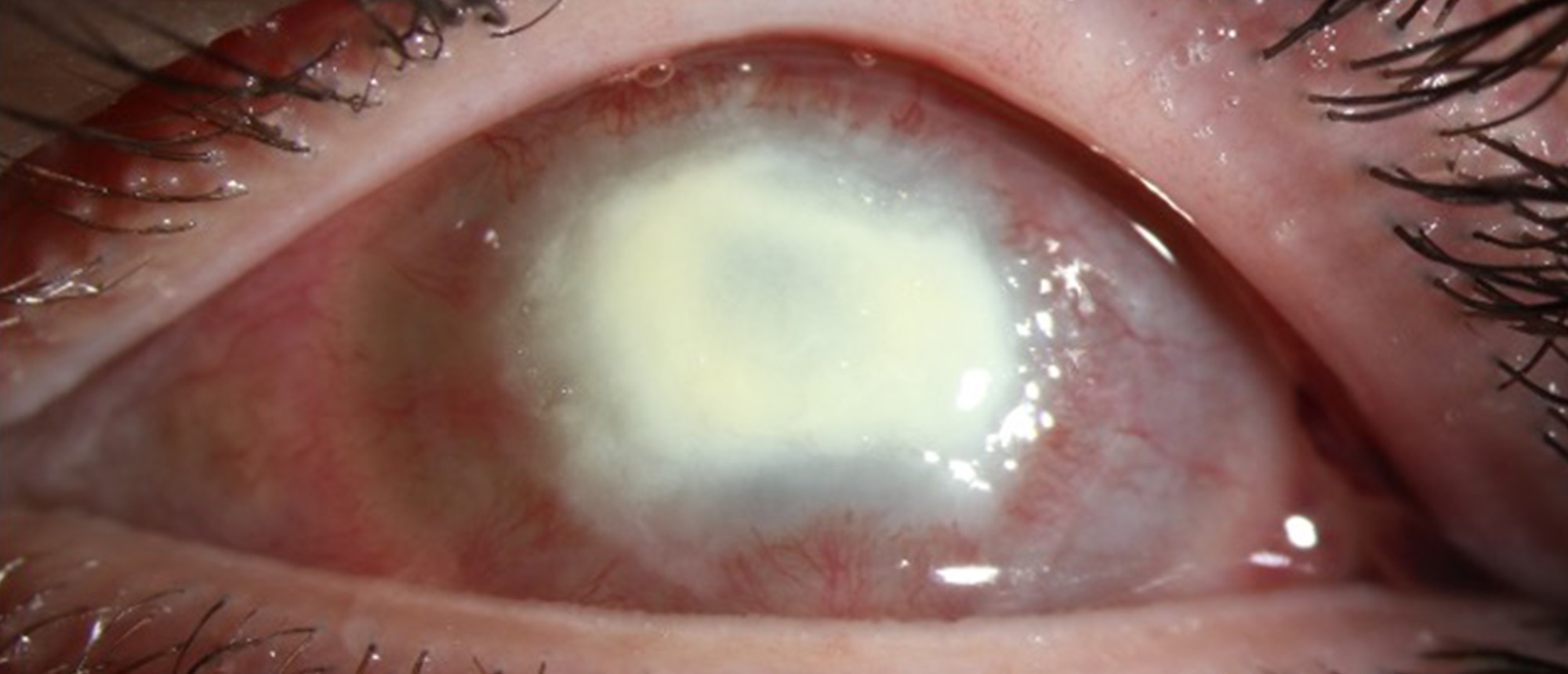
Acanthamoeba Keratitis
A patient presented to the BPEI emergency room with left eye redness and pain for 2 weeks. He had been diagnosed with HSV keratitis by an outside provider but had no improvement on valacyclovir. The vision was 20/20 in the right eye and 20/60 in the left eye, and intraocular pressures were normal. The exam was notable for a healed corneal epithelial defect and corneal haze, and the patient was started on topical steroids. Two weeks later, he re-presented with a ring infiltrate and significant corneal haze and AC inflammation. Confocal microscopy was inconclusive, but cultures returned positive for Acanthamoeba. The patient was started on polyhexamethylene biguanide and chlorhexidine, as well as topical steroids and moxifloxacin. However, the patient’s pain and clinical condition worsened, and he subsequently underwent Rose-Bengal photodynamic therapy with a conjunctival flap. In the post-operative setting, his pain worsened with the appearance of further corneal melting. The decision was made to perform a therapeutic penetrating keratoplasty, and the patient was taken to the operating room, but a corneal sample was found to have no cysts intraoperatively and the stroma appeared fuller than previously described. Therefore, the TPK was aborted, and a corneal scrape with AMT was performed instead. In the following week, the patient’s pain improved and the corneal infiltrate began to consolidate. Culture returned negative. Over the next several weeks, the patient continued to improve, with complete consolidation of the infiltrate and resolution of the KED. A corneal graft for visual rehabilitation will be considered in the next few months.
Presentation Date: 06/08/2023
Issue Date: 06/23/2023
Please log in or click on ENROLL ME to access this course.