
Intraorbital Foreign Body
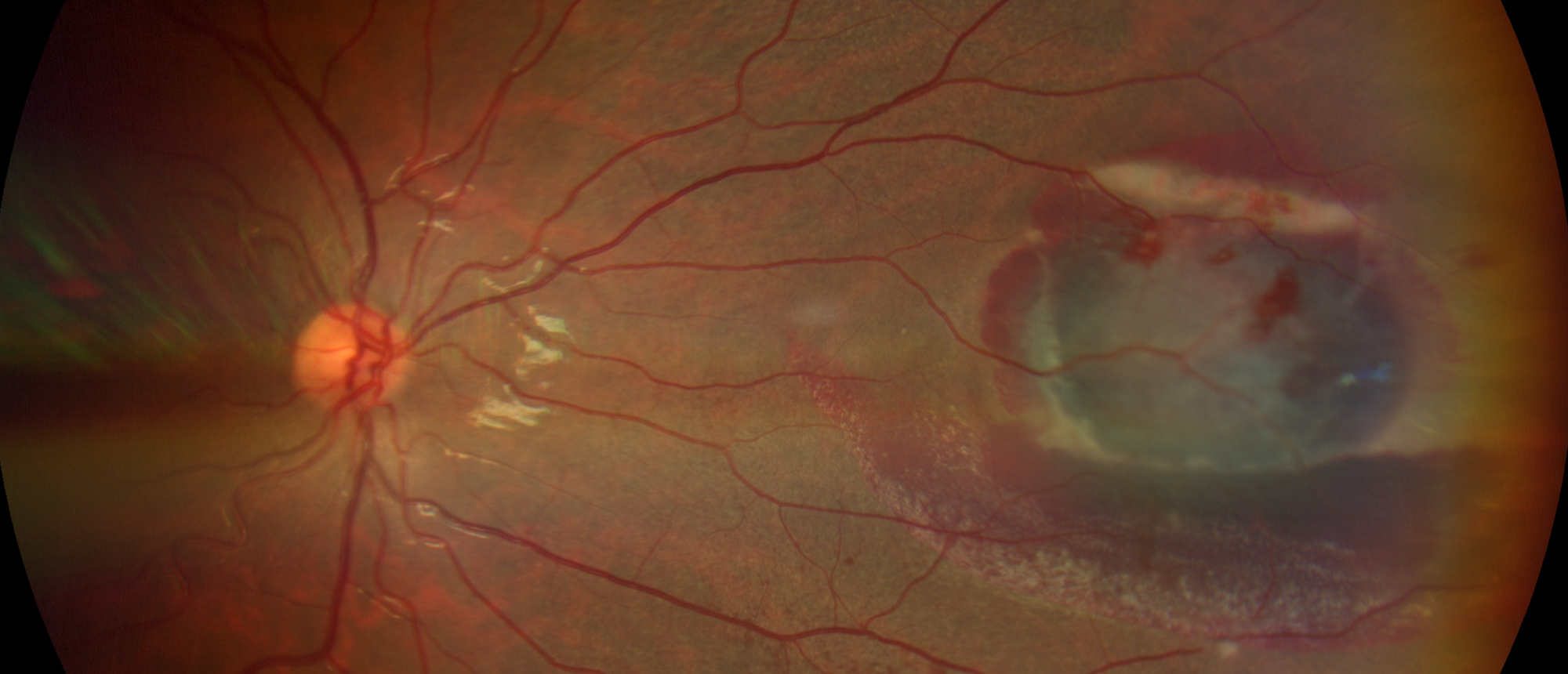
Intraorbital foreign bodies most commonly present with an ocular or penetrating injury. However, when the globe is not involved, the presentation of an intraorbital foreign body can be subtle. Here, we present a case of a 21-year-old female with right upper and lower lid swelling after allegedly sustaining an air injury from an unloaded pellet gun. Exam revealed no evidence of globe rupture or compromise in visual function; a dilated fundus exam did reveal an area of subretinal fluid with surrounding intraretinal heme in the peripheral retina. This significant posterior injury did not seem to correlate with the patient’s reported mechanism of injury. A CT scan was thus obtained which led to the diagnosis of a retrobulbar metallic intraorbital foreign body. Physicians should have a high index of suspicion for an intraorbital foreign body based on the patient’s history and mechanism of injury. CT scan remains the gold standard for screening intraorbital foreign bodies because it can characterize the type of foreign body and, unlike MRI, can safely detect metallic foreign bodies. While surgical management is typically employed on a case-by-case basis, the type, location, and secondary complications of an intraorbital foreign body often dictate surgical removal versus close observation. Organic and copper intraorbital foreign bodies must be surgically removed due to their high risk of infection and inflammation. On the other hand, inorganic foreign bodies can often safely remain in the orbit with close observation. Complications that would necessitate surgical removal include optic neuropathy, intracranial extension, restriction of ocular movements, infection, and inflammation.
Presentation Date: 12/10/2020
Issue Date: 06/25/2021
Please log in or click on ENROLL ME to access this course.
