
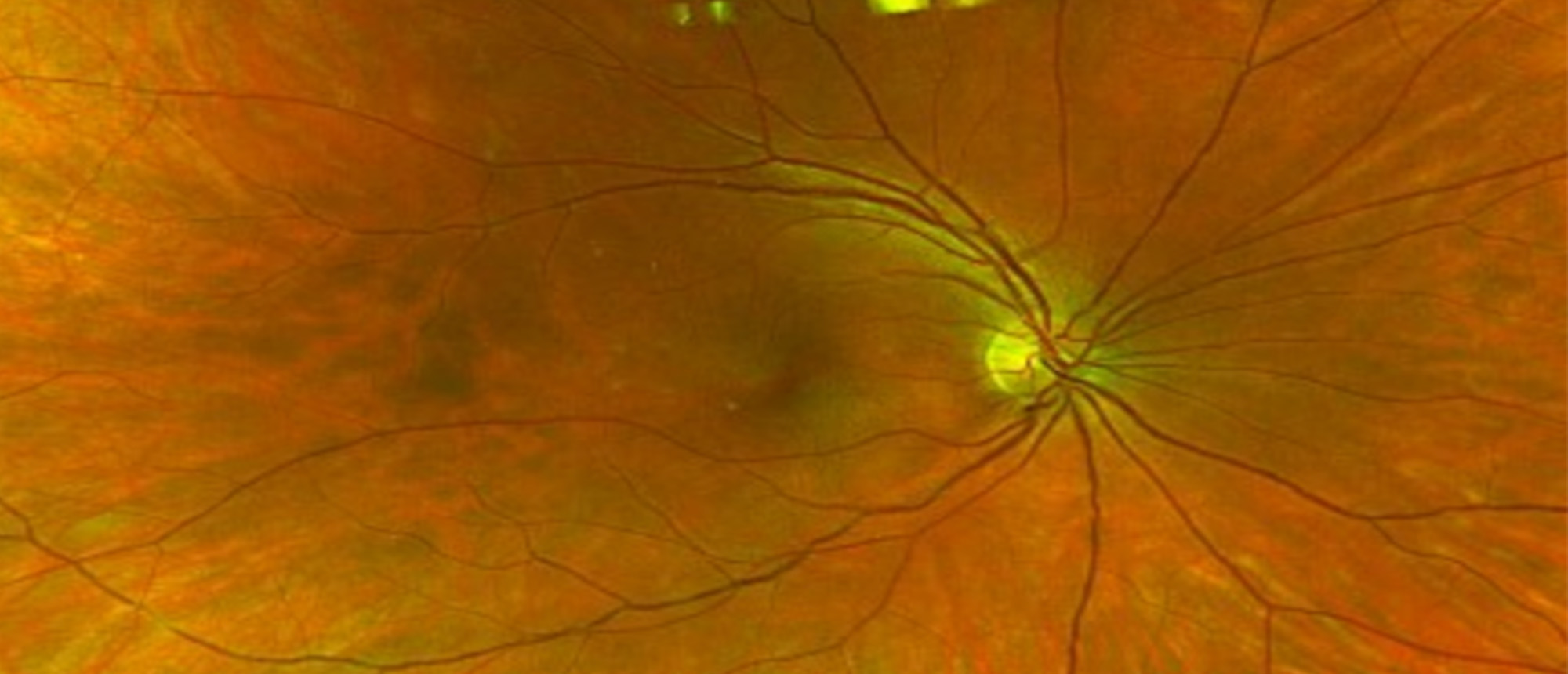
Birdshot Chorioretinopathy
A patient with blurred vision and uveitis was referred to the Bascom Palmer Eye Institute, Naples. She had received a sub-tenon steroid injection in the left eye. On examination, visual acuity was 20/20 in both eyes. Fluorescein angiography (FA) revealed venous leakage, and indocyanine green angiography (ICGA) showed multiple hypocyanescent lesions at the choroidal level. Laboratory testing was positive for HLA-A29, while other infectious and inflammatory markers were negative. She was diagnosed with birdshot chorioretinopathy (BSCR) and treated with systemic mycophenolate mofetil 1000 mg BID. BSCR is a bilateral, non-granulomatous autoimmune disease usually limited to the eyes. The most frequent visual symptom is blurred vision. On examination, anterior segment inflammation is typically mild or absent. Mild vitritis is also a common finding. Fundus examination shows yellow, creamy lesions at the choroidal level radiating from the optic nerve. FA shows large venule leakage, and ICG typically shows hypocyanescent lesions. HLA-A29 is positive in 95% of cases. Cystoid macular edema is a common OCT finding in these patients. This disease is progressive and, without treatment, results in loss of visual function. Treatment includes control of acute symptoms with local steroids. Long-term disease control can be achieved with immunomodulatory therapy and biologic medications. Visual field testing and ERG are useful modalities for monitoring disease activity.
Presentation Date: 05/29/2025
Issue Date: 04/24/2026
Please log in or click on ENROLL ME to access this course.
