
Paralytic and Restrictive Medial Rectus Dysfunction Secondary to Cocaine-Induced Midline Destructive Lesions
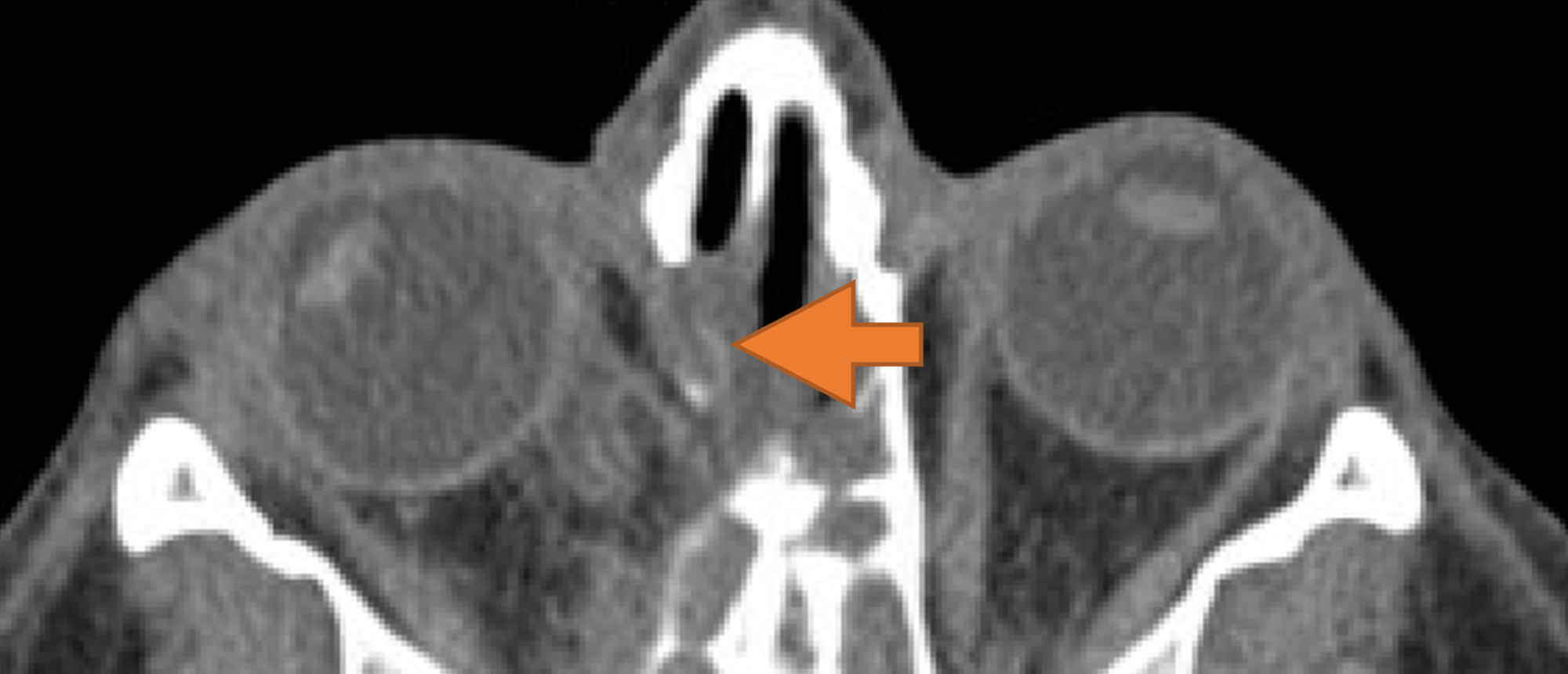
A patient with a history of prolonged cocaine abuse, recurrent orbital cellulitis and progressive sinonasal destruction presented with right exotropia for two years and diplopia for one year, alleviated with patching. There was no prior strabismus surgery. Examination demonstrated good visual acuity in both eyes and a large-angle right exotropia with marked limitation of adduction. Forced duction testing revealed significant restriction to adduction, which improved after lateral rectus disinsertion, suggesting a combined restrictive and paretic process. Imaging demonstrated absence of the nasal septum and inferior turbinates with medial orbital scarring. Further questioning revealed chronic intranasal cocaine abuse, consistent with cocaine-induced midline destructive lesions. A combined oculoplastic and strabismus surgical approach was undertaken. Extensive scar tissue tethering the medial rectus was released, followed by medial rectus resection and lateral rectus recession. Although initial alignment improved, residual exotropia with suspected paralytic medial rectus dysfunction persisted. A second procedure was performed consisting of additional lateral rectus recession and partial vertical rectus transposition. Postoperatively, ocular alignment improved significantly with restoration of stereopsis and resolution of diplopia, with residual limitation of adduction. This case highlights the importance of thorough history-taking, differentiation of restrictive versus paralytic strabismus, and staged surgical management in complex extraocular muscle injury associated with cocaine-induced sinonasal destruction.
Presentation Date: 03/05/2026
Issue Date: 03/27/2026
Please log in or click on ENROLL ME to access this course.
