
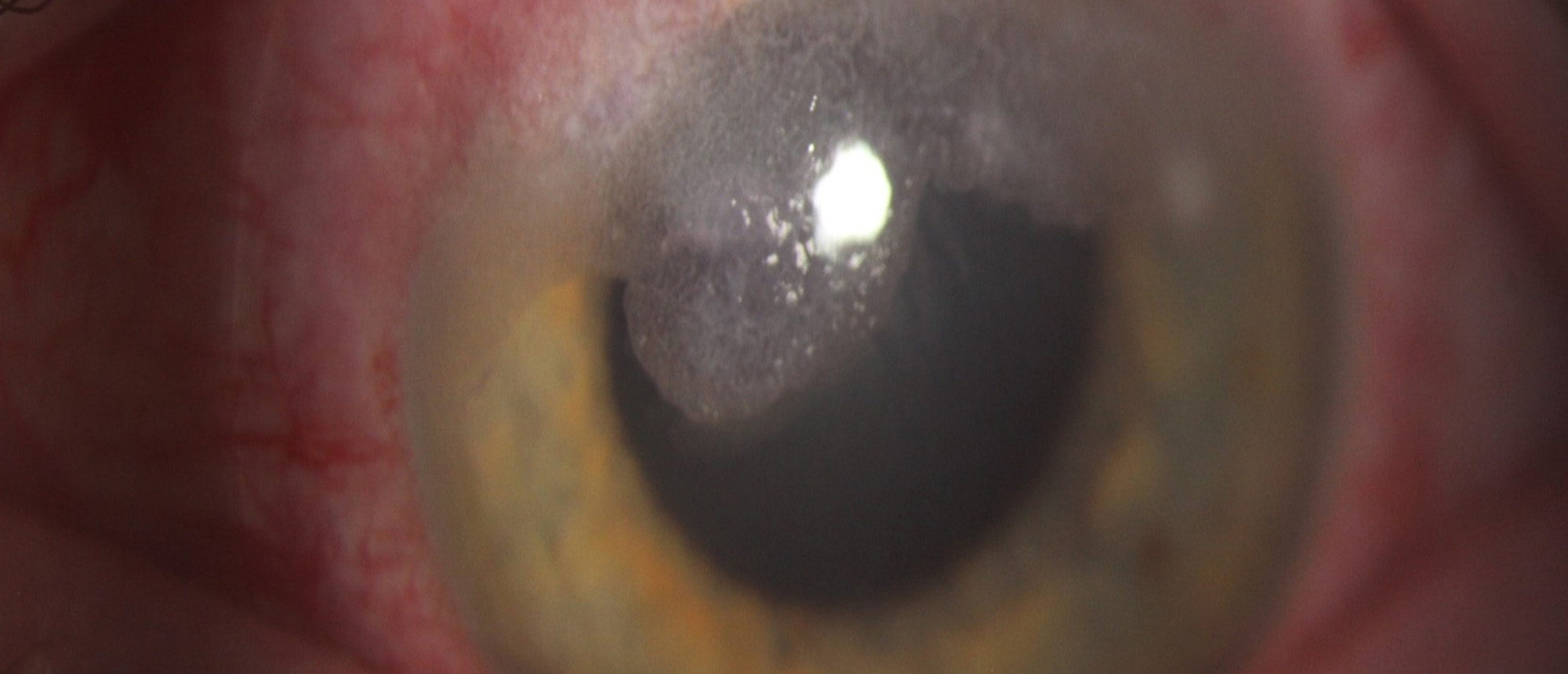
Terrien's Marginal Degeneration
A young patient presents to the ER with sudden discomfort in the left eye, immediately followed by tearing and blurred vision that took place at 11:00 am that day without an inciting event or trauma. He has no past medical history or ocular history. Vision is 20/15 in the right eye and 20/350 without correction in the left eye. Intraocular pressure was unreadable. On exam of the left eye, a superior horizontal 5mm area with lipid deposition and proximal thinning was noted with Seidel positivity and the anterior chamber was flat. Dilated fundus examination was normal. CT orbits without contrast did not note foreign body. The perforation was glued and a bandage contact lens was placed. The patient was started on hourly fortified antibiotic drops. In another second case, a young patient presents with superotemporal corneal thinning noted on routine ocular examination. Past medical and ocular history was non-contributory, and best corrected vision was 20/30 and 20/20 in the right and left eyes. Intraocular pressure was normal in both eyes. On exam, the patient had a pannus superiorly extending 2mm past the limbus with lipid deposition and stromal thinning without epithelial defect or area of perforation in the right eye. The left eye was normal. Dilated fundus examination was normal in both eyes. Anterior segment OCT of the right cornea showed superotemporal diffuse opacity with ~70-80% posterior stromal thinning and posterior stromal pseudocyst, but the overlying epithelium was smooth and intact. Topography showed irregular astigmatism in the right eye only. Diagnosis of Terrien's marginal degeneration was made in both eyes. The first patient after glue, bandage contact lens, and topical prednisolone and antibiotics improved to UCVA 20/20 in the affected eye. The second patient remained stable with topical prednisolone alone. Terrien's marginal degeneration is characterized by slowly progressive, unilateral or asymmetrically bilateral superior corneal thinning that spreads peripherally, which can cause against the rule or oblique astigmatism. A hallmark of the condition is lipid deposition at the leading edge of the affected area of corneal thinning. There is usually an absence of inflammatory signs or symptoms. There are two postulated subtypes of Terrien's marginal degeneration that are highlighted by these two cases: first being inflammatory, noted by ocular pain, injection, photophobia, and fluorescein staining, that can eventually lead to spontaneous perforation. The second subtype is degenerative, which is slowly progressive with lack of symptoms and fatty degeneration of the stromal lamella due to idiopathic tissue hypoxia. Generally, treatment is conservative, limited to glasses, scleral lenses, or RGP contact lenses, but perforation should be managed with patch graft when necessary.
Presentation Date: 02/26/2026
Issue Date: 03/27/2026
Please log in or click on ENROLL ME to access this course.
